

Isoniazid
By S. Knut. Chadwick University.
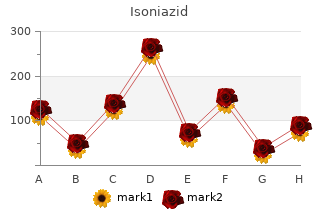
Asimismo cheap 300 mg isoniazid fast delivery treatment knee pain, se propone comunicar los resultados consensuados e instruir a la población de usuarios y a los responsables de toma de decisiones, con el fin de promover modificaciones respecto a la reserva de desincriminación de la tenencia de hojas de coca para el coqueo. Fifty-four patients with medically intractable epilepsy were investigated (40 patients with partial epilepsy and 14 patients with primary generalized epilepsy). The acquisition parameters were the following: A non-circular orbit, 64 steps, 30 s each, filtered back projection (Shepp-Logan-Hamming filter) was used for the reconstruction o f transverse slices; no attenuation correction was performed. An unambiguous pathological scintigraphic pattern was detected in 11 patients; ten o f them revealed a perfusion defect and a significant hyperperfused area was present in one patient. The findings in the other 13 patients were highly suspicious o f perfusion changes (in seven patients hypoperfusion and in six patients hyperperfusion zones). The application of various radiopharmaceuticals represents probably the last, but not the least, possibility of epileptic focus detection. Increased perfusion of an epileptic focus during partial epileptic paroxysm was shown for the first time by Ingvar in 1973 [1]. He also reported that in the interictal state the focal area had a decrease in flow to below the normal level. However, the methodology using intra-arterial application of the inert gas 133Xe is rather com plicated and therefore not suitable for routine clinical practice. We have become very interested in epileptic patients during the last three years and almost 60 patients have been examined with diagnosis of epilepsy. One patient was injected ictally and the others were investigated interic- tally (several patients post-ictally). Sagittal and coronal slices were also routinely reconstructed and evaluated, and the possi bility of semiquantitative analysis has been utilized in the last two years. All of them were treated with various anti-epileptic drugs (monotherapy in 20 patients, two anti-epileptics in 32 patients, and 2 patients took a combination of 3 drugs). This therapy had completely no effect on 35 patients, who suffered from several seizures per month or even per week. The neurological clinical status was normal in 52 patients, and light hemiparesis was found in two patients. The findings in 13 other patients (24%) were highly suspicious of perfusion changes — in 7 patients hypoperfusion and in 6 patients hyperperfusion zones (Figs 1 and 2). Localized defects of brain perfusion were revealed in 70% of the pathological cases and hyperperfused zones were detected only in seven patients (30%). This finding correlates with the fact that most of the patients were investigated interictally. Ten patients benefited from these procedures — seven of them became seizure- free after changing the therapy on the strength of correct localization of the focus, and three patients in our group have undergone successful neurosurgery intervention so far. The localization of extratemporal neocortical epileptogenic foci is more difficult than that of temporal lobe epilepsy. The final epileptogenic foci were considered as determined when either all three tests were concordant or two tests were in agreement while the remaining was non-lateralizing. The final epileptogenic focus was in the frontal lobe in eight patients, lateral temporal in six, parietal in three, occipital in three and undetermined in three patients. Epilepsies with partial seizures are divided into temporal lobe epilepsy and extratemporal (neocortical) lobe epilepsy. However, a very few reported studies in patients with neocortical epilepsy [3, 4]. All patients were admitted to the Seoul National University Hospital between September 1994 and May 1995. The acquisition was started not earlier than 30 min after tracer injection to allow sufficient washout from extracerebral tissue, and the acquisition time was 30 min. The final epileptogenic foci were considered as determined when either all three tests were concordant, or two tests were in agreement while the remaining were non-lateralizing. In the case of the thalamus, similar hyper- perfusion was found in 20% of the patients. These findings were common especially in patients with frontal and occipital lobe epilepsies (Table I). Most epilepsies with partial seizures are those with seizures presumably originating from a restricted, structurally abnormal cortical region and, therefore, are the epilepsies that might benefit from restrictive surgery [1]. If syndromatic subclassification is attempted, most probably two epilep sies with partial seizures can be distinguished.
In this case isoniazid 300mg free shipping medicine wheel, transbronchial needle aspiration of a hilar lymph node demonstrated noncaseating granulomas, as did transbronchial tissue biopsies. Even without overt involvement of lung parenchyma, granulomas are frequently found on transbronchial tissue biopsies. In this patient without symptomatic disease and normal lung function, no treatment is necessary. She should receive reassurance and close follow-up for development of symptomatic disease. In stage I disease, between 50 and 90% will resolve spontaneously without treatment. Usually doses of 20–40 mg are effective, but with cardiac or neurologic involvement, higher doses of prednisone, up to 1 mg/kg, are often necessary. For severe manifestations of sarcoidosis, addition of azathioprine, methotrex- ate, or cyclophosphamide may be required. This patient has no evidence of infection by clinical history, with a biopsy that is negative for fungal and mycobacterial organisms. At this point, management should focus upon establishing and maintaining blood pressure for adequate organ perfusion. Life-threatening anaphylaxis is an immediate IgE-mediated hy- persensitivity reaction that usually appears within minutes of exposure to a sensitized anti- gen. However, most individuals who die of anaphylaxis related to insect stings are unaware of their sensitization. Symptoms of anaphylaxis include urticaria, angioedema, laryngospasm, bronchospasm, and vascular collapse. With the onset of anaphylactic shock, massive vasodilatation and capillary leak occur. Additional doses can be given as needed every 5 min, and there is no absolute contraindication to ongoing treatment with epinephrine in anaphylaxis. If anaphylaxis fails to improve quickly with ad- ministration of epinephrine, establishment of a secure airway and delivery of oxygen should be paramount. Previous studies have demonstrated no differ- ence between colloid and crystalloid solutions for initial volume resuscitation in anaphylaxis. However, lactated Ringer’s solution should not be used because of an increased risk of meta- bolic acidosis. Other vasopressor ther- apy such as dopamine or vasopressin can be added to maintain blood pressure if the shock is refractory to epinephrine infusion. Antihistamine therapy with H1 and H2 blockers are con- sidered second-line therapy after epinephrine, as these agents have a slower onset of action. Antihistamine therapy alone should not be given for treatment of anaphylactic shock. Glu- cocorticoids have no role in the acute therapy of anaphylaxis, but should be administered once the patient is stabilized to prevent late-phase reactions with recurrent anaphylaxis. Dis- connecting the patient from the ventilator would be appropriate for the treatment of hy- potension due to the development of intrinsic positive end-expiratory pressure. In addition, it is noted that the wheezing stops prior to the next inhalation, suggesting that the patient is fully exhaling the inspired tidal volume. Specific therapies have been developed to target the inflammatory response to sepsis, particularly the effect of the inflammatory response on the coagulation system. This drug is an anticoagulant that may also have antiapoptotic and anti-inflammatory proper- ties. In a randomized controlled trial, activated protein C was associated with an absolute re- duction in mortality of 6. However, in those individuals who are less severely ill, activated protein C may increase mortality. While it is unethical to randomize individuals to a trial as- sessing the appropriate timing of antibiotic delivery, retrospective analyses have demon- strated an increased risk of death if antibiotics are not given within 1 h of presentation. A single-center trial of early goal-directed therapy in septic shock showed a survival advantage when this approach was taken. Early goal-directed therapy developed a protocol for fluid administration, institution of vasopressors, and blood transfusion based on physiologic pa- rameters, including mean arterial pressure, central venous oxygen saturation, and presence of acidosis among others. However, there is no evidence that bicarbonate improves hemodynamics, response to vasopressors, or outcomes in septic shock. He denies symptoms of the most common causes of chronic cough, such as asthma, gastroesophageal reflux disease, and postnasal drip.
Jonathan Unsworth-White Aspirin irreversibly inhibits platelet function by blocking the cyclooxygenase pathw ay generic isoniazid 300 mg otc 5 asa medications. It is a vital adjunct in the prevention of coronary throm bosis1 and is know n to reduce the risk of acute bypass graft closure. Therefore if aspirin w ere discontinued 10 days prior to surgery, the affected platelet pool w ould be com pletely replenished w ith fresh platelets by the tim e of the operation. This how ever leaves the patient vulnerable to an acute m yocardial event during the latter part of this tim e and m ay also m ake graft occlusion m ore likely in the im m ediate postoperative period. Collaborative overview of random ised trials of antiplatelet therapy-1: Prevention of death, m yocardial infarction, and stroke by prolonged antiplatelet therapy in various categories of patients. Pre-operative aspirin decreases platelet aggregation and increases post-operative blood loss – a prospective, random ised, placebo controlled, double-blind clinical trial in 100 patients w ith chronic stable angina. Tom Treasure There are three circum stances w hen surgery is required for m itral regurgitation: 1 To save life in the acute case Sudden m itral regurgitation follow ing rupture of degenerative chordae tendineae, papillary m uscle rupture, or endocarditis m ay be very poorly tolerated. The surgeon m ay be presented w ith a patient in pulm onary oedem a, even ventilated, and then an oper- ation m ay be the only w ay to save life. The decision is not alw ays easy but a sensible appraisal of the risks and benefits is w hat is needed. If there is a tolerably good ventricle, and substantial regurgitation to correct, then the benefits are likely to outw eigh the risks. The degree of left venticular dilatation to be tolerated before surgery is required has reduced. Som e patients seem to tolerate m itral regurgitation quite w ell w ith a large ventricle ejecting partly into a large, relatively low pressure left atrium. The left ventricle m ay not be as good as it appears because the high ejection fraction is into low afterload. Im pact of pre- operative sym ptom s on survival after surgical correction of m itral re- gurgitation. Robin Kanagasabay M itral valve repair has been popularised by Carpentier and others and now represents a recognised option in the treatm ent of m itral valve disease. Advocates argue that all m itral valves should be considered for repair first, and only those that are not suitable should be replaced. M itral valve repair offers real advantages over replacem ent, chiefly low operative risk (around 2% 1,2), avoidance of the risks of long term anticoagulation (in patients w ho are in sinus rhythm ), very low risk of endocarditis, and probably better long term preservation of left ventricular function. The last aspect m ay not be as clear cut as once thought as techniques to replace the m itral valve w hile still preserving the sub-valvular chordal apparatus, w hich is so im portant in regulating ventricular geom etry, m ay offer m any of the advantages once held to be the sole preserve of repair techniques. Repair of anterior leaflet prolapse is a m ore com plex undertaking and requires either a transfer of chordae from the posterior to the anterior leaflet, or the use of synthetic chordae. An alternative is to suture the free edges of the tw o leaflets together at their m id-points creating a double orifice valve, the so called Alfieri bow -tie repair. It m ay require a com bination of leaflet augm entation using patches of peri- cardium , and also elongation or replacem ent of any restricted chordae. Restricted leaflet m otion due to poor ventricular function rem ains a particularly difficult problem to correct by repair techniques. Features which indicate a low chance of successful repair These include: • Rheum atic valvular disease • Thickened valve leaflets • M ultiple m echanism s of valve dysfunction • Extensive prolapse of both leaflets • Com m issural regurgitation • Annular calcification • Dissection of valve leaflets com plicating endocarditis. In general all valves that can be repaired should be, although som e patients m ay opt for valve replacem ent to avoid the (sm all) risk of needing further surgery due to failure of the repair. Because of the low operative risk, absence of the need for anticoagulation and avoidance of the risks of prosthetic valve endocarditis follow ing valve repair, a further group of patients m ay be offered valve repair at an early stage of their disease w here, on the balance of risks, valve replacem ent w ould not yet be justified. Long-term results of m itral valve repair for m yxom atous disease w ith and w ithout chordal replacem ent w ith expanded polytetrafluoroethylene sutures. Superiority of m itral valve repair in surgery for degenerative m itral regurgitation. Cost im plications of m itral valve replacem ent versus repair in m itral regurgitation. The Ross procedure, or pulm onary autograft procedure, w as introduced by M r Donald Ross in 1967. The principle is to replace the diseased aortic valve w ith the autologous pulm onary valve.
Prazosin has a slow onset (2–4 h) and a long duration of action (10 h) and is extensively metabolized by the liver (50% during first pass) generic isoniazid 300mg with visa treatment yeast infection child. Labetalol (Normodyne and Trandate) (1) Labetalol is a competitive antagonist (partial agonist) that is relatively selective for a1-receptors and also blocks b-receptors. Phenoxybenzamine (Dibenzyline) (1) Phenoxybenzamine is a noncompetitive, irreversible a1-receptor antagonist. Overview (1) a1-Adrenoceptor antagonists are used most often to treat hypertension and urinary obstruction of benign prostatic hypertrophy. Pheochromocytoma (1) Pheochromocytoma is a tumor of the adrenal medulla that secretes excessive amounts of catecholamines. Adrenoceptor antagonists, particularly labetalol, are occasionally used to reverse hyperten- sive crisis due to sudden increase in a-receptor stimulation (e. Tamsulosin may have greater efficacy due to its selective action at a1A-receptors. Adverse effects of phentolamine include postural hypotension, reflex tachycardia, arrhyth- mia, angina, and diarrhea. This drug should be used cautiously in patients with a peptic ulcer or with coronary artery disease. Prazosin, terazosin, and doxazosin produce postural hypotension and bradycardia on initial administration; these drugs produce no significant tachycardia. Labetalol produces fewer adverse effects on the bronchi and cardio- vascular system than selective b-receptor antagonists. Chapter 2 Drugs Acting on the Autonomic Nervous System 49 (4) Initially, they may increase peripheral resistance. However, long-term administration results in decreased peripheral resistance in patients with hypertension. Respiratory system (1) b-Adrenoreceptor antagonists increase airway resistance as a result of b2-receptor blockade. Eye (1) b-Adrenoreceptor antagonists decrease the production of aqueous humor, resulting in reduced intraocular pressure. Including propranolol, many have low bioavailability (<50%) because of extensive first-pass me- tabolism; marked interpatient variability is seen, particularly with metoprolol. Propranolol (Inderal) (1) Propranolol is a competitive antagonist at b1- and b2-receptors. Metoprolol (Lopressor), betaxolol (Betoptic), bisoprolol (Zebeta), atenolol (Tenormin), acebutolol (Sectral), and esmolol (Brevibloc) (1) These drugs are somewhat selective b1-receptor antagonists that may offer some advantage over nonselective b-adrenoceptor antagonists to treat cardiovascular disease in asthmatic patients, although cautious use is still warranted. Labetalol (Normodyne and Trandate), Carvedilol (Coreg) (1) Labetalol is a partial agonist that blocks b-receptors and a1-receptors (3:1 to 7:1 ratio). Carvedilol also has mixed activity but is equiactive at b-receptors and a1-receptors. Timolol (Blocadren), levobunolol (Betagan), nadolol (Corgard), and sotalol (Betapace) (1) These drugs are nonselective b-receptor antagonists. Pindolol (Visken), carteolol (Cartrol), and penbutolol (Levatol) are nonselective antagonists with partial b2-receptor agonist activity. Cardiovascular system (see also Chapter 4) (1) b-Adrenoreceptor antagonists are used to treat hypertension, often in combination with a diuretic or vasodilator. Long-term use of timolol, propranolol, and metoprolol may prolong survival after myocardial infarction. This effect is thought to be related to the slowing of ventricular ejection and decreased resistance to outflow. Eye (1) Topical application of timolol, betaxolol, levobunolol, and carteolol reduces intraocular pressure in glaucoma. Other uses (1) Propranolol is used to control clinical symptoms of sympathetic overactivity in hyper- thyroidism by an unknown mechanism, perhaps by inhibiting conversion of thyroxine to triiodothyronine. All agents (1) b-Adrenoreceptor antagonists should be administered with extreme caution in patients with preexisting compromised cardiac function because they can precipitate heart fail- ure or heart block. Nonselective adrenoceptor antagonists (1) These drugs may cause bronchoconstriction, and thus they are contraindicated for asth- matics.
8 of 10 - Review by S. Knut
Votes: 50 votes
Total customer reviews: 50